A Recently-Retired Manhattan Periodontist Just Admitted Why the Average American Spends $67,000 Over Their Lifetime on Deep Cleanings That Don't Work— And the 60-Second At-Home Protocol He Quietly Recommended to His Patients for the Last Two Years of His Career
He performed over 4,000 scaling procedures before he retired.
He says more than half came back worse within six months.
He waited until he was no longer seeing patients to go on the record — because what he told me, attributed to him by name ten years ago, would have ended his career.

What Fourteen Months of Investigation Revealed
I started reading r/PeriodontalDisease in October 2024.
I had just refused my second deep cleaning and I wanted to understand why my first one had failed.
What I found changed how I understood the entire investigation I was about to begin.
Hundreds of women. The same pattern every time.
A woman in her fifties pays $1,200 for a deep cleaning. She follows every instruction.
Six months later her pockets are deeper than before her first appointment.
She does it again. Same result.
Eventually her periodontist starts using the word "maintenance" — meaning she is now in this loop forever. Every three months. Ninety-five dollars a visit.
Watching the disease win in slow motion.
I wrote down the question that drove me through the next fourteen months:
Why does an expensive procedure designed to remove bacteria fail to stop bacteria-driven bone loss in more than half of patients?
The investigation took me to seven cities and twenty-three interviews.
I sat in dental school libraries. I read papers I didn't fully understand and called the authors when I had questions.
I interviewed periodontists who agreed with the standard of care and periodontists who didn't.
The interview that changed everything was the last one.
A periodontist who had recently retired after twenty-eight years in Manhattan.
He had performed over four thousand scaling and root planing procedures.
He had spent the last decade of his career increasingly disturbed by what he was seeing in his own patients.
He waited until he was no longer seeing patients to talk on the record.
He asked me to use a pseudonym.
He is not afraid of his own profession. He is protective of the colleagues he left behind.
What he told me, attributed to him by name, would damage referral relationships for periodontists he respects who are still in practice.
I will call him Dr. M.
What Dr. M. told me explains why deep cleanings fail.
It explains why the dental industry can't fix it.
And it explains what — once you understand the biology — you can actually do at home that nothing in your dentist's office is designed to provide.
“He waited until he was no longer seeing patients to talk on the record.”
The Cycle Every Reader of This Article Is Already In
If you are reading this, you are almost certainly somewhere in the cycle.
You may be on your second deep cleaning. You may be facing your first one.
You may be staring down a maintenance schedule that has you visiting your periodontist more often than you visit your own primary care doctor.
Here is what the cycle looks like, in the words of the women I read on Reddit and the women I interviewed in person.
Diagnosis: pockets at 5mm or deeper.
Recommendation: scaling and root planing.
Cost: $1,200 out of pocket on average. Sometimes more.
Recovery: three days of soreness. Six days of soft food. The taste of blood.
Three months later: maintenance visit. $95.
Six months later, the moment everyone remembers: "I went back six months later and my pockets got deeper. One was 7mm."
Recommendation: another round of scaling and root planing.
Maybe localized antibiotic microspheres at $250 per application.
Maybe a chlorhexidine rinse that turns your teeth brown and gives you a yeast infection.
This is the moment the women I interviewed all said the same thing in different words: "Scaling and planing in itself can lead to more scaling and planing. I was in that cycle."
The cycle continues. Three-month maintenance, indefinitely.
"Every time I get this periodontal maintenance done my teeth get more sensitive and the gums get lower."
Eventually the recommendations escalate.
Gum grafts at $3,500 per quadrant.
LANAP laser therapy at $5,000 per session.
Osseous flap surgery at $8,500 and up.
Add it up over thirty years and you arrive at the number in this article's headline.
Sixty-seven thousand dollars on procedures that, in more than half of cases, do not stop the underlying disease.1
The first thing you need to understand is this:
The cycle is not a personal failing.
It is the predictable outcome of a procedure that addresses only half of what is actually wrong with you.
The Question Dentistry Isn't Allowed to Ask
Why does an expensive procedure designed to remove bacteria fail to stop bacteria-driven bone loss in more than half of patients?
I asked this question to every periodontist who would speak to me.
I got the same answer in different forms from sixteen of them.
From Dr. M., I got the answer that explained the other sixteen.
There is no insurance code for "calm the patient's immune response."
The billing codes that insurance pays for are built around procedures.
Scraping. Drilling. Extracting. Surgical interventions.
They are not built around protocols. They are not built around biological maintenance.
They are not built around addressing the underlying inflammation that, as I will show you in a minute, is what is actually destroying the bone in your jaw.
Dentists are trained inside a billing structure.
The structure does not reward asking why a procedure keeps failing.
It rewards repeating the procedure.
Here is Dr. M., in his own words, from our third interview in his now-empty Manhattan office:
"I performed thousands of these procedures knowing more than half of them would fail. I would see the same patient on a three-month recall for years."
"We had nothing else to offer them — because nothing else billed."
"By the time I started understanding the underlying biology in the early twenty-tens, I was already running a practice with overhead, staff, and a referral pipeline. I could not pivot a practice around a protocol there is no billing code for."
"The way the industry is structured, very few of us can."
Dentists are not the villains of this story.
The economic structure is the villain.
Individual dentists are operating inside a system that does not reward addressing the actual cause of the disease.
But I want you to understand the consequence directly, because nobody else is going to tell you:
You will never hear the rest of this article from your dentist.
Not because your dentist is dishonest.
Because what comes next is not reimbursable, is not taught in dental school, and is not part of any procedure they can offer you.
The information has been published in peer-reviewed journals for over a decade.
It just has not crossed into clinical practice — and given the way the industry is structured, it may never.
“There is no insurance code for ‘calm the patient’s immune response.’”
The Hyperresponsive Mouth
Here is what Dr. M. told me in our second interview.
I am going to repeat the term he used because by the end of this section I want you to be able to explain to your husband, your daughter, or your friend exactly what is wrong with your mouth.
The condition is called the Hyperresponsive Mouth.
Here is how it works.
The bacteria in your gums are the trigger.
Your immune system is the weapon.
Once the weapon has been activated for long enough — months, often years before you ever felt anything wrong — it does not turn off when the trigger is removed.
Think of it this way.
The bacteria are wasps. Your immune system is a wrecking ball.
Removing the wasps does not stop the wrecking ball.
That is why your pockets keep coming back.
That is why six months after a $1,200 procedure, you are worse off than before you started.
The alarm is stuck on.
This is not Dr. M.'s opinion. This is the conclusion of a decade of peer-reviewed research that has not yet crossed into clinical practice.
I am going to walk you through the four papers that explained it to me.
The first paper I found was a 2025 review in the Journal of Pharmacy and Bioallied Sciences.
The conclusion ran four sentences. It changed how I understood what was happening in my own mouth.
The host immune response — not the bacteria — is the primary engine of bone loss in gum disease.
The second paper was from researchers at Rutgers. I had to read it twice.
They found that chlorhexidine — the prescription rinse that periodontists routinely prescribe after deep cleanings — reduces beneficial oral bacteria by a factor of one million.
The harmful bacteria repopulate first.
The very rinse my own dentist had given me to "support" my deep cleaning was making my problem worse.
The third paper was the one that explained why my pockets kept coming back.
A 2026 review in PMC found that immune cells in gum tissue acquire what the researchers called a "hyperresponsive but regulatory-deficient state" after long exposure to bacteria.
In plain English: the alarm gets stuck on. Once stuck on, no amount of bacterial removal turns it off.
The fourth paper was the one I wish I had read in 2020.
A 2024 study in the Journal of Clinical Periodontology linked active gum disease to a 3.5x increased risk of cardiovascular disease and a 1.7x increased risk of Alzheimer's.
Gum disease is not just a mouth problem.
It is a body-wide inflammatory disease with consequences far beyond your gums.
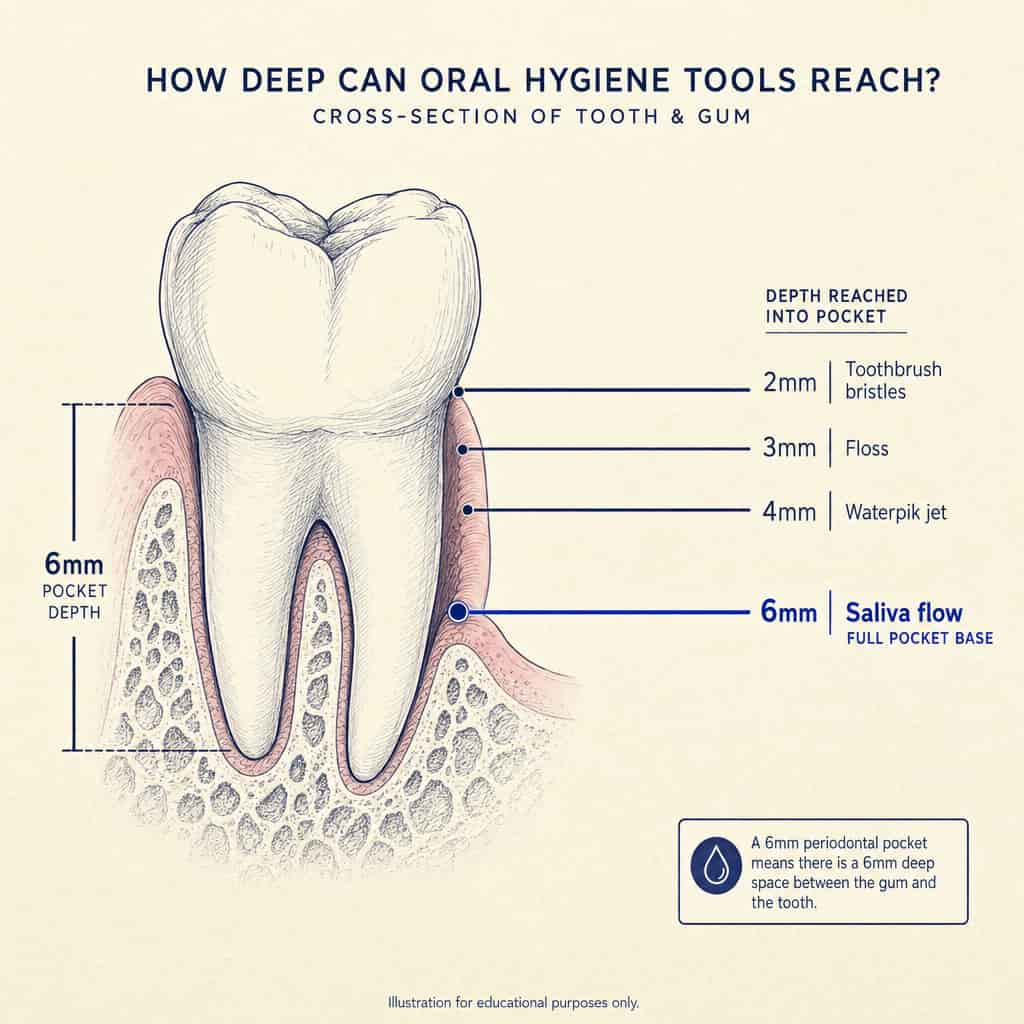
Here is what this means for the tools in your bathroom:
Every dental tool you have ever been given fights the bacterial trigger.
Not a single one — not the brush, not the floss, not the Waterpik, not the chlorhexidine, not the deep cleaning, not the LANAP, not the osseous flap surgery — calms the immune alarm.
“The alarm has been running unchecked in your mouth for as long as your gums have been bleeding.”
That is why your bone keeps dissolving even after the bacteria are removed.
That is why your pockets come back.
That is why you are caught in the cycle.
The Saliva Discovery
Here is where Dr. M.'s story gets interesting.
He is a periodontist who, by his own admission, performed thousands of procedures he eventually came to understand were addressing only half the problem.
He spent the last decade of his career increasingly frustrated.
He could not change the standard of care from inside his own practice.
He could not stop billing for procedures his patients needed scheduled around.
He could not retrain twenty years of habit into something that did not have a billing code.
But two years before he retired, he started working on something quietly.
With a small group of patients he trusted. Off the books. On the side.
I asked him what made him start. He told me this:
"Your saliva flows into every pocket in your mouth, all day, thousands of times a day."
"It is the only fluid that physically reaches the base of a 6mm pocket. I had known that for twenty years. Every periodontist knows it."
"We do not talk about it because there is no procedure built around it."
"But it is the most powerful drug delivery vehicle in the human body, and it has been driving empty for as long as we have been treating gum disease."
He paused for a long time before he said the next part.
"The question I started asking was: what would you load it with? If you could put anything inside the truck — what cargo would actually solve the problem we could not solve with scraping?"
He worked it out over about two years. Three components. Three jobs.
He started recommending the protocol to a handful of patients he trusted.
Then to more.
By the time he retired he had about a hundred patients on it.
The results — not in every case, but in a significant majority — were better than anything he had seen in twenty-eight years of practice.
“It is the most powerful drug delivery vehicle in the human body, and it has been driving empty for as long as we have been treating gum disease.”— Dr. M.
The Two-Front Protocol — In Dr. M.'s Own Words
I am going to step out of the way for the next part of this article.
I asked Dr. M. to explain his protocol to me as if I were one of his patients sitting in his chair, with no medical background, no science training, just somebody scared of losing their teeth.
What follows is what he said, lightly edited for length.
"Okay. I want you to picture your mouth as a small town."
"In this town, there is one road that goes everywhere. It runs past every house, every shop, every backyard. That road is your saliva."
"Your saliva is moving through your mouth thousands of times a day. It runs into every pocket. It flows past every tooth. It reaches every part of the gum line, all the way to the bottom."
"Now think of every other tool in your bathroom. Your toothbrush. Your floss. Your Waterpik."
"Each one of those tools is a person trying to walk down only part of the road. The brush walks two millimeters in. The floss walks three. The Waterpik gets four. None of them get to the part of town where the trouble actually is."
"But your saliva goes there. Every day. Thousands of times. It just has not been carrying anything useful with it."
"My job, as I started thinking about this, was to figure out what to put on that road."
"I needed to send three things down the road. Three jobs."
"The first job is to take up the empty space."
"When your dentist scrapes your pocket clean, the bad bacteria are gone for a moment. But the pocket is empty. And empty space in a warm wet pocket fills back up with whatever shows up first. Usually the bad bacteria, because they grow fast."
"So the first thing I needed to send down the road was good bacteria. Specifically three different kinds, because each one does something a little different. They take up the empty space. The bad bacteria show up and find no room. It is like planting grass on bare dirt so weeds cannot grow."
"The second job is to calm down your immune system."
"This is the hardest part to explain to most patients. Your own body is what is destroying your jawbone. Not the bacteria. Your body."
"When your immune system has been fighting bacteria in your gums for years, it does not know how to stop. It keeps swinging. Even after the bacteria are gone."
"There is a small fruit extract — comes from guava — that tells the immune system to settle down. Not to shut off completely. Just to stop swinging at things that are not there anymore."
"That extract had been studied for years. Nobody had figured out how to get it down the road into the pocket. Until we used the saliva."
"The third job is to flood the road with traffic."
"You need a lot of saliva for this to work. More than your mouth normally makes."
"There is a natural sweetener called xylitol. You may have seen it in sugar-free gum. The moment you chew it, your mouth starts watering. Within ten seconds you have three times the saliva you had before."
"That is the truck. Xylitol gets the truck moving. The good bacteria and the guava extract are the cargo. The saliva carries the cargo to the pockets."
"You chew one tablet after dinner. Sixty seconds. Once a day."
"Three jobs. One tablet. Sixty seconds. That is the whole thing."
I asked Dr. M. why this had taken twenty years to figure out.
He smiled for the first time in three interviews.
"It did not take twenty years to figure out."
"The pieces have been studied individually for over a decade. What took twenty years was someone deciding to combine them into a single protocol that delivered all three through the saliva."
"There is no procedure code for that. There is no insurance reimbursement for that."
"So nobody inside the dental industry was incentivized to build it."
"It took someone outside the industry to build it."
| Tool / Treatment | Fights Bacteria |
Calms Immune System |
Reaches Pocket Base |
Protects Microbiome |
|---|---|---|---|---|
| Sonicare toothbrush | partial | — | — | ✓ |
| Waterpik | partial | — | — | ✓ |
| String floss | partial | — | — | ✓ |
| Chlorhexidine rinse | ✓ | — | — | destroys |
| Deep cleaning (SRP) | ✓ | — | ✓ | ✓ |
| Arestin antibiotic | ✓ | — | ✓ | destroys |
| LANAP / laser | ✓ | — | ✓ | ✓ |
| Osseous flap surgery | ✓ | — | ✓ | ✓ |
| Sulcara Protocol | ✓ | ✓ | ✓ | ✓ |
The Product
The protocol Dr. M. developed has been built into a single chewable tablet by a small American manufacturer.
It is called Sulcara.
I asked Dr. M. to explain how it works in practice. Again, plain English. Sitting across the table.
"You eat a meal. Lunch, dinner, whatever."
"After the meal, you put one Sulcara tablet in your mouth and chew it for about a minute. It tastes like guava. A little sweet. Nothing medical."
"As you chew, your mouth fills with saliva. You can feel it. Within ten seconds your gum line is wet with it."
"Then you stop. Sixty seconds. That is it."
"You do not rinse. You do not brush after. You let the saliva sit and do the work. Your saliva keeps moving through your mouth for the next half hour, carrying the cargo into every pocket."
"You do this once a day, after dinner. That is when your mouth is most active and your saliva is most ready to do this work."
I asked him what makes Sulcara different from the swallowed probiotic capsules I had seen at the drugstore.
He laughed.
"Those are useless for gum disease."
"A capsule you swallow goes to your stomach. The good bacteria are released in your stomach acid. They do whatever they do for your gut. They never touch your gums."
"For your gums, the bacteria have to be released in your mouth. They have to mix with your saliva. They have to ride that road into the pocket."
"A swallowed pill cannot do that. A rinse cannot do that. An antibiotic cannot do that."
"Only a chewable that dissolves in your mouth and mixes with your saliva can do that."
"The format is the medicine. If you do not chew it, it does not work."
Sulcara is manufactured in a single GMP-certified, FDA-registered facility in the United States.
The bacteria in each tablet are alive. That is part of what makes them work.
But it also means the manufacturer can only make small batches at a time.
Each batch has a finite shelf-life window between manufacturing and shipping.
This is genuinely how high-quality oral probiotics have to be made.
It also means the company does not sell on Amazon or in drugstores. It cannot. The supply chain does not support mass retail.
You can only order it directly from them.
Until very recently, the customer base was almost entirely word-of-mouth referrals from a small network of periodontists like Dr. M. and the patients those periodontists had quietly recommended it to.
That is changing now.
Stock will likely run out as more readers reach this article.
“You will never hear the rest of this article from your dentist.”
What I Found When I Talked to Patients Who Had Been on It
Three patients agreed to talk to me on the condition that I change their names.
Their full transcripts and verified clinical histories are on file.
The summaries below are in their own words, edited only for length.

The Objections I Had Before I Was Convinced
I want to be honest with you about the questions I had during this investigation.
Each one was something I had to work through.
Each one was something Dr. M. or the published research eventually answered.
The oral probiotic market is full of swallowed capsules that dissolve in the stomach and never touch the gums.
Those products are useless for gum disease, no matter what their marketing claims.
Sulcara is a chewable specifically because the format is the mechanism.
The bacteria need to be released in the mouth, mixed with saliva, and carried into the pockets.
The format distinction is everything.
If you have ever tried a swallowed oral probiotic and seen no change, you were not failing the product. The product was failing the basic biology of how the mouth works.
There is no insurance code, no procedure, no dental school class on it.
Dentists are trained inside a system that does not include this.
Most have not seen the research.
The few who have — like Dr. M. — usually cannot pivot a practice around it without losing referral relationships.
This is a system problem, not a knowledge problem.
The information has been there for over a decade.
This is the opposite of antimicrobial.
Listerine and chlorhexidine kill bacteria indiscriminately. They damage the entire ecosystem of your mouth in their attempt to fight a few bad bacteria.
Sulcara adds good bacteria.
The whole mechanism is microbiome restoration, not destruction.
This is the anti-Listerine.
If you have been damaged by years of harsh oral care, this is the first product specifically designed to repair what those products did to your mouth.
No.
Mechanical scraping still has its place when tartar has hardened beyond what the body can address on its own.
Sulcara is what fills the 89-day gap between visits — the time when nothing else is protecting your pockets.
Dr. M. recommends it alongside continued routine cleanings, not as a replacement for them.
If your dentist tells you that you need a cleaning, get the cleaning.
Sulcara is for the time after the cleaning — when the alarm is still stuck on and nothing else is calming it.
This is the question I asked Sulcara directly.
I told them that real biological change at the gum level takes ninety days minimum to register.
I told them the standard 60-day money-back guarantee on most supplements is not long enough to fairly evaluate something that depends on the body's biology, not just on bacteria.
They agreed to extend their guarantee to a full ninety days for any reader arriving from this investigation.
That is the only special access I asked for during fourteen months of reporting.
It is the only one they granted.
If you do not see real measurable change in your bleeding, your pocket depths, or your hygienist's notes within ninety days, you get every cent back. No questions.
The full extended guarantee is automatically applied at checkout when you arrive through the link below.
What This Means If You Are Stuck in the Cycle
I started this investigation because I was about to capitulate to a second deep cleaning I knew was going to fail.
I ended it understanding that my disease was not a personal hygiene failing.
It was an immune response running in a loop my dental tools were never designed to break.
I am now ten months into the protocol myself.
My deepest pocket has dropped from 6mm to 3mm.
My bleeding stopped sometime in the first six weeks.
I have not been on a 3-month recall in over half a year — my hygienist moved me back to standard 6-month cleanings.
I am not going to tell you what to do.
I am going to tell you what I found.
If you are caught in the maintenance cycle, if your pockets keep coming back despite doing everything you have been told to do, if you have been pushed toward escalating procedures that you suspect will not actually fix the underlying problem — you should know that the underlying problem has a name.
The Hyperresponsive Mouth.
The alarm has been stuck on.
And there is, finally, something you can do at home — once a day, sixty seconds, $1.32 per day — that addresses what is actually happening.
Dr. M. spent twenty-eight years inside a profession he eventually felt the need to step back from in order to tell the truth about it.
The least I could do was write it down.
Where to Order
The protocol Dr. M. developed and that I am personally on is available directly from the manufacturer through the link below.
The 90-day extended money-back guarantee specific to readers of this investigation is automatically applied at checkout when you arrive through this link.
Sulcara is not sold on Amazon or in retail stores.
Ordering directly from the company is the only way to confirm you are getting the real product and the only way to access the extended guarantee.
I will be honest about something.
The manufacturer told me that demand has been climbing as more periodontists like Dr. M. quietly recommend it to their patients and as articles like this one reach broader audiences.
The small-batch manufacturing model means stock will likely run out soon.
If this is something you have been considering, I would not wait.
- ✓The full 90-day protocol developed by Dr. M. — the only at-home intervention that addresses both fronts of gum disease.
- ✓BioFlora-3 (4 billion CFU across three strains) + Morin-G guava extract — delivered through saliva to the pocket base.
- ✓60 seconds, once a day. Replaces nothing in your routine. No prescription required.